
Caso presentado en la edicion 174 por Jaime Piquero Martin y Edgar La Rotha Higueras.
Clínica de la piel. Clínica Sanatrix. Caracas Venezuela
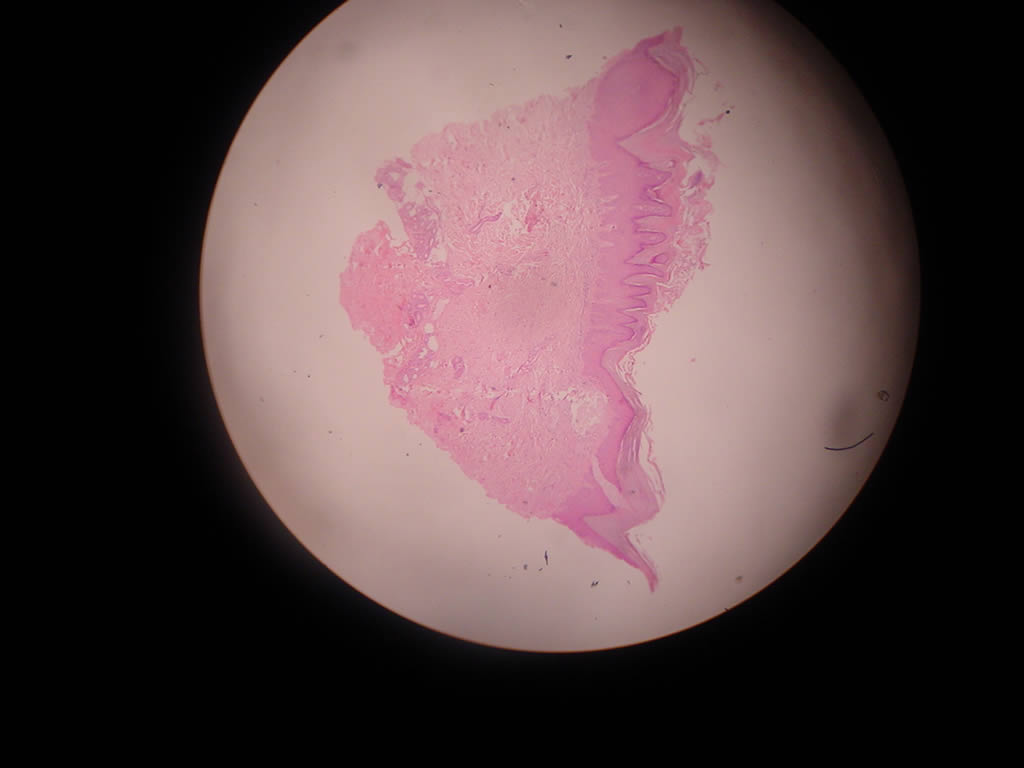
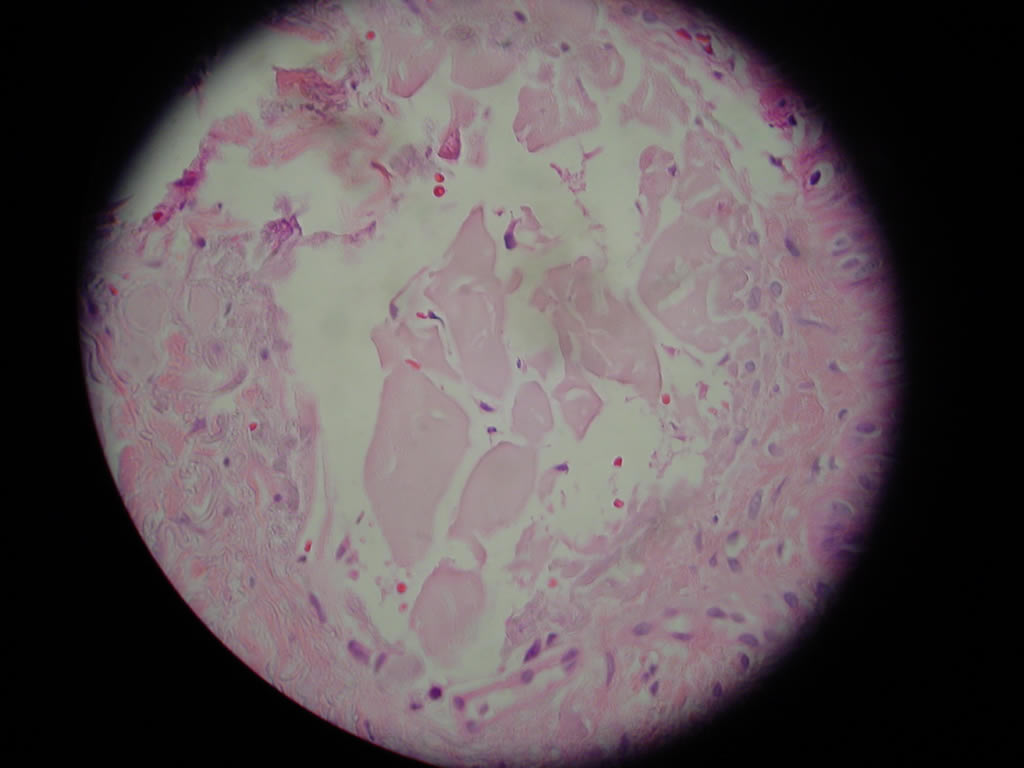
Recordarán que presentamos a un paciente de 38 años fototipo II motorizado, con importante fotodaño que presenta en dorso de manos y antebrazos pápulas que confluyen formando placas que le dan a la piel de la zona un aspecto “correoso”. Se aprecian algunas pápulas que semejan quistes de inclusión. Se toma biopsia la cual es reportada como Enfermedad de depósito probablemente Amiloide ( Rojo congo positivo).



Enfermedad de depósito
¿ Es un liquen amiloideo?
¿ El daño actínico tiene alguna incidencia en la etiología en este paciente?
¿ Como podríamos ayudarlo?
La coloración para rojo congo resulto POSITIVA
Hice un analisis del caso que llevamos a consideración de ustedes, descartamos en principio los diagnósticos de Liquen amiloide por no tener el aspecto caracteristico, a pesar que la coloracion para rojo congo resulto positiva, pero nos basamos en el trabajo enviado por el DR. Guillermo Planas ( ver abajo).
La posibilidad de foliculitis perforante inducida por daño solar Crónico aunque presenta un material amorfo que emerge en unos cortes la clínica esta muy lejos de ella .
Igual podriamos decir de la Acroqueratosis verruciforme que asoma nuestro amigo Aldo Gonzalez
Me gusta el diagnóstico de milium coloide que sugiere Guillermo , ya que al ver al paciente en mi consultorio me habia pasado por la mente.
El planteamiento de sugerencias para su manejo siguen en pie
Nota : Las fotos y analisis en cuadro son remitidas gentilmente por el Dr. Guillermo Planas
Images
|
||||||||||||||||||||||||||||||||||








Differential Diagnosis
|
||||||||||||||||||||||
Discussion
Lichen amyloidosis and colloid milium both result from deposits of homogeneous material in the dermis, but the composition chemical of them is as different as the appearance of them histopathologically. In both conditions, fibrocytes are affiliated closely with the deposits of homogeneous material. In fact, it is likely that fibrocytes are responsible for the formation of amyloid in lichen amyloidosis and of colloid in colloid milium.
Because of the highly characteristic attributes histopathologic conditions, just listed, specialized stains need not be performed routinely to differentiate between amyloid and colloid. When necessary for academic resolution of the issue in a particular instance, Congo red is the most reliable stain for differentiation because it is positive by dichroism for amyloid and negative for colloid. Crystal violet stain for amyloid is prettier and more dramatic, but less reliable.
The lesion clinical of lichen amyloidosis consists of agminated, discrete, slightly raised, brownish-red translucent papules that often are keratotic. The condition is intensely pruritic and occurs most commonly on the anterior aspects of the legs, but in some circumstances may be widespread. Macular amyloidosis, as the title implies, consists of flat lesions. In contrast to lichen amyloidosis, macular amyloidosis has a predilection for the interscapular region. The keratotic papules of lichen amyloidosis are consequent not only to progressive accumulation of amyloid in the papillary dermis, but to the effects of persistent rubbing as well. In short, superimposition of lichen simplex chronicus on macular amyloidosis transforms that condition into lichen amyloidosis. The evidence for that is prominent compact orthokeratosis and hypergranulosis in virtually all lesions of lichen amyloidosis, signs incontrovertible of persistent, prolonged rubbing. Macular amyloidosis that has not been rubbed and, therefore, not thickened by lichen simplex chronicus, remains flat, as is the case stereotypically in the interscapular region. A current hypothesis about how amyloid comes to be deposited in the upper portion of the dermis in lesions of macular amyloidosis and lichen amyloidosis holds that globules of amyloid derive from necrotic keratocytes in the epidermis, they being secondary to the effects of scratching, and when those bodies are acted on by fibrocytes, amyloid is the result.
Colloid milium consists of discrete, smooth, yellowish, translucent, waxy papules on sun-exposed sites, especially the malar eminences of the face and dorsa of the hands. Sometimes the papules of colloid milium are restricted to the left side of the face and the dorsa of the left hand in persons who spend much of their time driving a car in a sunny climate, such as is the situation for taxi drivers. At first glance, the smooth translucent papules of colloid milium may be misinterpreted as tense vesicles or as "juicy" edematous papules of polymorphous light eruption. Histopathologically, colloid is surrounded always by copious amounts of solar elastosis, both of them being stained bluish-gray by hematoxylin and eosin. That concurrence and those findings indicate that colloid and elastotic material are related closely to one another. Amyloid, by contrast, is not in any way associated with damage by sunlight.
Whereas colloid in the skin is found only in colloid milium, amyloid is detected in a variety of circumstances other than in the macular and papular (lichenoid) forms. For example, amyloid is present around blood vessels in the skin and subcutaneous fat of patients with systemic amyloidosis, in large solitary nodules of nodular amyloidosis and, most often as a finding incidental in a host of inflammatory, hamartomatous, and neoplastic conditions in the skin, especially in seborrheic keratoses, trichoepitheliomas, and basal-cell carcinomas. In those conditions, individual keratocytes tend to undergo necrosis.
Search Derm101.com for lichen amyloidosis and colloid milium.
Sin lugar a dudas se trata de un milium coloide, la clínica, el antecedente de exposición solar, la localización dan el diagnóstico. Si se pide una nueva tinción con Azul alcian quedará mejor demostrado.
Tenemenos recopilado unos 8 casos aproximadamente de milium coloide, de los cuales la localización principal fue el dorso de manos y antebrazos, solo uno tubo en tórax,era un agricultor que trabaja a torso desnudo. Si hay oportunidad les puede hacer llegar las fotografías. Hemos presentado esto en alguno de los CILADs o RADLAs si no mal recuerdo.
DR. EDUARDO GARZÓN ALDÁS
DERMATÓLOGO.
HOSP. DERMATOLÓGICO GONZALO GONZÁLEZ
QUITO-ECUADOR