
Dr. José María Ollague Torres Dermatólogo – Dermatopatólogo
Servicio de Dermatologia “Dr. Wenceslao Ollague L.” Hospital de IESS Guayaquil – Ecuador
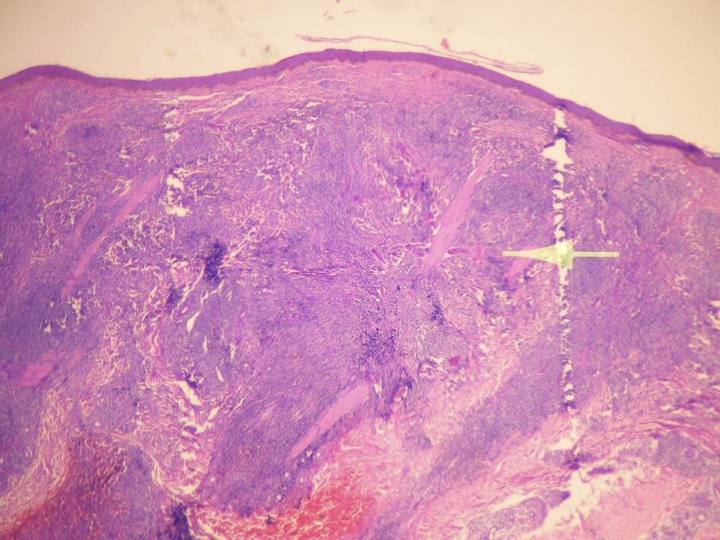
Historia: julio 2006. Paciente mestizo de 49 años residente en guayaquil- vendedor, sin antecedentes de importancia. Desde hace tres meses presenta lesion única, asintomático, eritemato-violacea de 2 cm. En su mayor diámetro discretamente infiltrada, localizada en antebrazo izquierdo. Buen estado general
Se toma biopsia (Ver ésta) y se concluye; LINFOMA DE CELULAS T CENTROFOLICULAR
- NOTA: ( LA POSIBILIDAD DE UNA HIPERPLASIA LINFOIDE DEBERIA CONSIDERARSE).
- El paciente desaparece por dos años ( Próxima edicion, continuación)




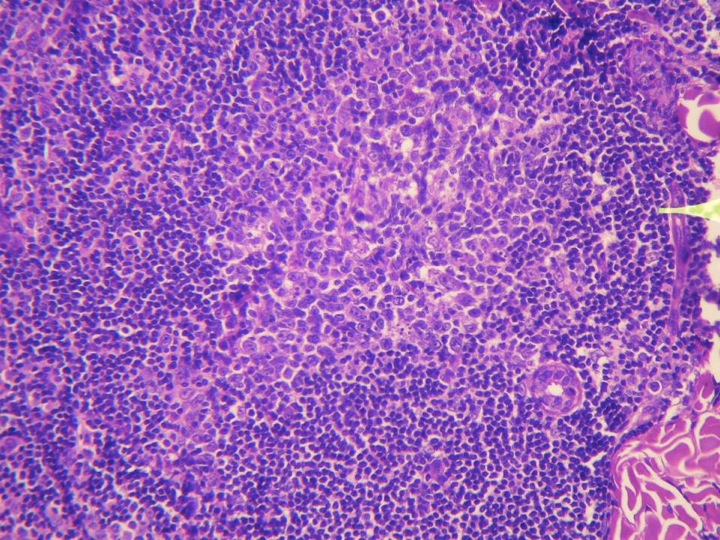
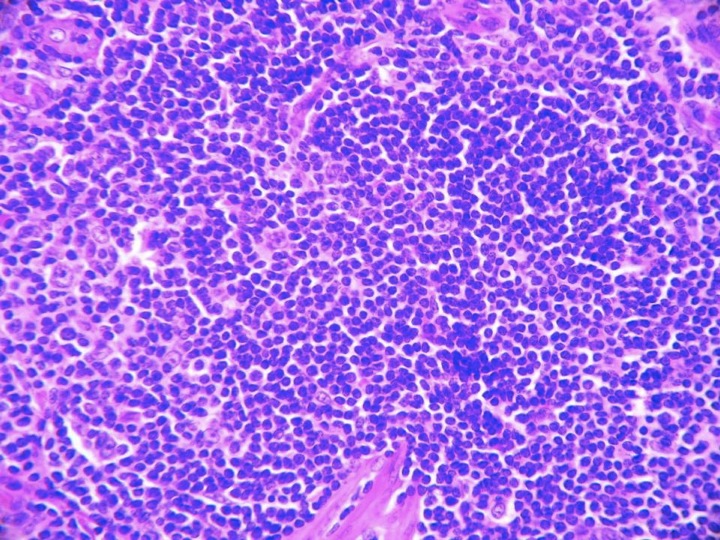

Estimado amigo: La biopsia muestra una lesión linfoide nodular con patrón folicular. Yo completaría el estudio inmunohistoquímico con blc-2 y bcl-6 para evaluar la posibilidad de linfoma centrofiolicular primario vs hiperplasia. Hemos visto casos similares en pacientes adultos jóvenes asociados a infección por Borrelial y H. pylori. Esperamos el seguimiento.
apenas llevo 3 meses en la especialidad,agradezco su paciencia, me parece un linfoma B pues hay una banda de colágena normal en la dermis papilar y es CD20+
Hay un error de tipeo en el diagnóstico, es Linfoma de Células B (no T) centrofoliculares.
Me adhiero a agregar Bcl2 y Bcl6 a la inmunomarcación, también haría CD10.
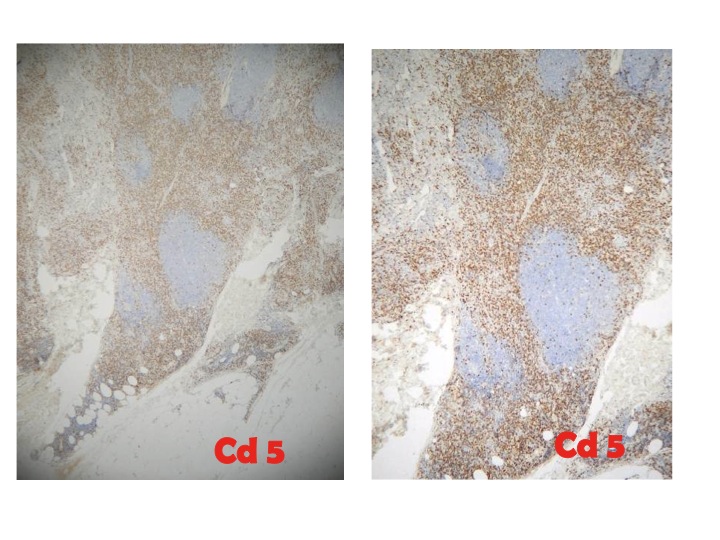
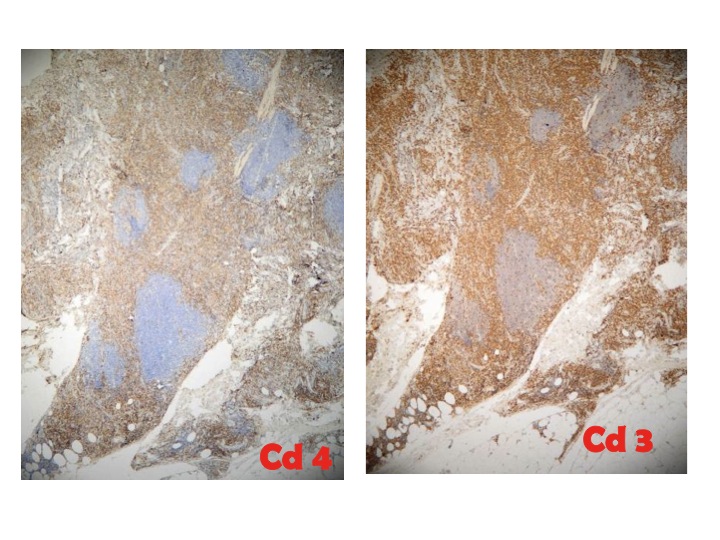
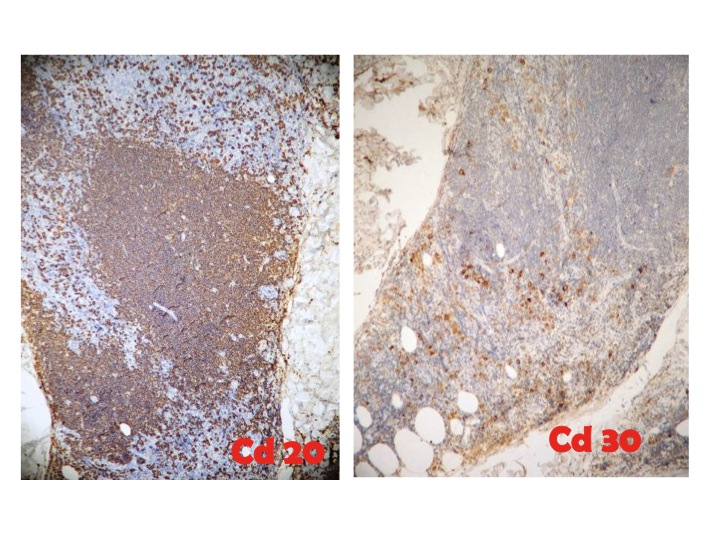
Querido Sergio, caso educativo y polemico, nos se ha realizado la marcacion bcl 2 ni el CD 10, ambos no estan a nuestro alcance, pero la impresion en H&E es la de una lesion linfoproliferativa de patron folicular muy localizada y demitada. la inmunomarcacion muestra CD 20+ solo en los cntros germinativos, Pero el esto del infiltrado es CD 3+, CD 4+, CD5+ y algunas de las celulas grandes anaplasicas fuera de los foliculos marcan para CD 30+ siendo estas la mayoria. El diagnostico de linfoma cutaneo de celulas B con patron folicular es casi obvio, sin embargo hay algunas publicaciones en la literatura que hablan de linfomas cutaneos primarios de celulas T con patron centro-folicular. Trataremos de hacer contactos pata hacer las marcaciones sugeridas separar una proliferacion maligna de una benigna sin embargo El Bcl 2 pareceria no ser tampoco muy buena para separar malignidad de benignidad
te adjunto dos referencias del tema:
Immunoreactivity for bcl-2 protein in cutaneous lymphomas and lymphoid hyperplasias.
Triscott JA, Ritter JH, Swanson PE, Wick MR.
Lauren V. Ackerman Laboratory of Surgical Pathology, Washington University Medical Center, St. Louis, Missouri, USA.
Comment in:
• J Cutan Pathol. 1995 Oct;22(5):476-8.
Abstract
The B-cell leukemia/lymphoma gene (bcl-2) produces a unique protein product (BCLP) that is believed to protect lymphoid cells from apoptosis. The bcl-2 gene is frequently rearranged in nodal follicular lymphomas as well as in diffuse lymphoproliferations, but has generally been regarded as most useful in the recognition of the former of these lesions. However, little is known regarding BCLP expression in cutaneous lymphoid infiltrates. Using an immunohistochemical technique and a monoclonal antibody (clone no. 124) the authors examined 67 examples of cutaneous lymphoid infiltrates–31 cases of malignant lymphoma of the skin (MLS) and 36 examples of cutaneous lymphoid hyperplasias (CLH)–to determine if patterns of BCLP reactivity could distinguish CLH from MLS or primary from secondary involvement of the skin by malignant lymphoma. Fifty-eight per cent of MLS cases were BCL-positive, as were 33% of CLH. Three of four cases of follicular cutaneous lymphoma showed BCLP-positivity in neoplastic follicles, whereas similar structures in cases of CLH with a follicular pattern were BCLP-negative. Sixty per cent of primary MLSs and 57% of secondary lymphomas were reactive for BCLP. These data suggest that immunostains for BCLP are of little help in the separation of benign from malignant cutaneous lymphoid infiltrates, and that they are likewise incapable of separating primary from secondary MLS. BCLP immunostains may have a limited adjuvant diagnostic role in distinguishing reactive from neoplastic follicular lymphoid lesions of the skin.
J Cutan Pathol. 1999 Jan;26(1):6-12.
Mainly unmutated V(H) genes rearranged in B cells forming germinal centers in a cutaneous pleomorphic T-cell lymphoma.
Golembowski S, Gellrich S, Lorenz P, Rutz S, Audring H, Sterry W, Jahn S.
Department of Dermatology, Medical Faculty (Charité), Humboldt-University Berlin, Germany.
Abstract
B cells in skin lesions of a pleomorphic cutaneous T-cell lymphoma with reactive germinal center hyperplasia were analyzed for their immunoglobulin V(H)DJ(H) gene rearrangements by micromanipulation and single cell polymerase chain reaction (PCR) analysis. In B lymphocytes located in germinal center-like structures, we found in 11/16 different V(H)DJ(H) rearrangements completely unmutated VH genes, suggesting that those cells did not undergo antigen-driven selection. Two V(H) genes showed more than 98% germ-line identity. In only three cells V(H) segments were somatically mutated to a higher extent, but two of these rearrangements were non-productive. These results differ markedly from what we have previously detected in B cells present in mycosis fungoides, another entity of cutaneous T-cell lymphomas where the Ig gene repertoire resembles the situation in peripheral blood with a significantly higher proportion of mutated V(H) genes. When investigating the large atypical B cells strongly expressing CD30 which were detected within the T-cell zone outside the germinal centers, we found again, in most cases, that the rearranged VH genes were completely unmutated. The B cells were of polyclonal origin. Due to this comparable Ig gene repertoire and mutational pattern, we suggest that these cells descend from the germinal center centroblasts which migrated into the T-cell zone and obviously became stimulated to express the CD30 marker. The micromanipulation technique and molecular analysis on the single cell level may provide an important input into our understanding of the mechanisms of immune regulation in cutaneous lymphomas.
Un abrazo pero hay mas despues con este caso
Estimada Veronica, gracias por el comentario, la zona de Grenz, efectivamente es muy sugestiva de una prolifercion de linaje B, pero los criterios para el diagnostico son tantos y tan complejos, el inmunomarcaje que pareceria que daria muchas luces en estos asuntos solo logra resolver algunos casos pero muchos otros muestran una confusion tremenda y el tiempo pasa hasta que puedan ser clasificados o reclasificados – lea el comentario sobre el Bcl 2. Me alegro y la felicito, siga adelante y no le tema a las confusiones que arman o armamos algunos mayores en el afan de encontrar un nombre y un comportamiento para un cuadro clinico.
Caro; el error -si es que lo hay – fue a proposito para generar algo de discusion y razonamiento- Gracias.